
Kidney Cancer
What Do the Kidneys Do?
The kidneys are essential organs that form part of the genito-urinary system. The kidneys filter the blood and the waste products are transferred through the ureters to be stored in the bladder as urine. Urine is then discharged through the urethra to empty the bladder.
The kidneys also produce three important hormones: erythropoietin (EPO), which triggers the production of red blood cells in bones; renin, which regulates blood pressure; and vitamin D, which helps regulate the body’s metabolism of calcium necessary for healthy bones.
How common is Kidney Cancer?
In Australia, kidney cancers account for just over 3% of all malignancies diagnosed in men and women each year.
Causes and Risk factors for Kidney Cancer
We don’t know what causes most kidney cancers. But some factors may increase your risk of Kidney Cancer.
These risk factors include:
- being a male,
- older age,
- obesity or having a body mass index (BMI) of 30 or more,
- smoking – the more you smoke, the greater the risk,
- high blood pressure (hypertension),
- family history – kidney cancer can be associated with an inherited genetic disposition, and
- end stage renal failure or long-term dialysis patients,
- a lack of physical exercise
What are the Symptoms of Kidney Cancer?
In many cases, there are no obvious symptoms at first however some symptoms can include:
- blood in urine – darker than usual or reddish in colour
- a persistent pain in your lower back or side, just below your ribs
- a lump or swelling in your side (although kidney cancer is often too small to feel)
Types of Kidney Cancer
There are several types of cancer that can affect the kidneys.
Renal cell carcinoma (RCC), is the most common form and accounts for approximately 85% of all kidney cancers. In Renal cell carcinoma, malignant cells develop in the lining of the kidney’s tubules and typically grow into a mass called a tumour. The most common subtype is called clear cell renal cell carcinoma (up to 75%).
Single tumours are the norm, although more than one tumour can develop within one or both kidneys.
As with most cancers, kidney tumours discovered at an early stage often respond well to treatment. The earlier kidney tumours are discovered, the better patient’s chances for survival. Survival rates in such cases are very high.
Tumours that have grown large or metastasised (spread) through the bloodstream or lymphatic system to other parts of the body are much more difficult to treat and present a greatly increased risk for mortality.

Gross Appearance of Kidney Cancer
Stages of Kidney Cancer
As discussed with other malignancies, the stage of renal cell carcinomas (RCC) is assigned by the tumour (T) , node (N) and metastases (M) classification systems:
There are 4 stages depending on the size of the cancer and whether it has spread or not, these are:
Stage 1: Kidney Cancer (T1, N0, M0)
Any T1 tumour without lymph node spread or metastases. Also referred to T1 Tumours, they are confined to the kidney without evidence of local invasion; no lymph node involvement and absence of distant disease.
- T1 a are those that are <4cm.
- T1 b are those that are between 4 and 7cm.

Small Renal Mass on CT Scan
Stage 2: Kidney Cancer (T2, N0, M0)
Any T2 tumour without lymph node spread or metastases. T2 Tumours confined to the kidney larger that 7cm with no evidence of local invasion; no lymph node involvement and absence of distant disease
Stage 3: Kidney Cancer
Either of these conditions:
– A tumour of any size in the kidney with a spread to the surrounding lymph nodes but not to other parts of the body (T1 or T2, N1, M0).
– The tumour has grown into the renal vein, and/or the vena cava (the main vein that carries blood from the body back to the heart) or perinephric tissue and may or may not have spread to regional lymph nodes. It has not spread to other parts of the body (T3, any N, M0).

Large Kidney Tumour on CT Scan
Stage 4: Kidney Cancer
Either of these conditions:
– The tumour has spread to areas beyond Gerota’s fascia and extends into the adrenal gland on the same side, possibly to lymph nodes, but not to other parts of the body (T4, any N, M0).
– The tumour has spread to any other organ, such as the lungs, bones, liver or the brain (any T, any N, M1).
Kidney Cancer Diagnosis
In order to accurately determine whether or not a patient has cancer, both
- a physical examination and
- a number of other tests
are required so that the doctor can rule out any other condition.
CT or MRI Scan
CT scans are special X-rays that show the internal organs of your body. Dyes (contrast) would conventionally be injected for accurate assessment, allowing the doctor to see the area more clearly. MRI scan is employed in cases of concern about contrast allergy, renal impairment, radiation exposure or equivocal findings especially for complex cystic tumours.
Urine tests (Urinalysis)
Nearly half of all patients with renal cell carcinoma (RCC) have haematuria or blood in their urine. Often this blood is present in such small amounts or is so diffused in the urine that it cannot be seen with the naked eye (called microscopic haematuria).
On occasion, cells found in the urine are examined under a microscope for abnormalities. This procedure is called urine cytology. This is typically indicated in patients at risk of urothelial cancer (cancer in the urinary tracts from the collecting system in the kidney, ureter and bladder)
Blood tests
Another routine investigation typically used in the diagnosis of RCC involves microscopic examination and/or chemical analysis of the patient’s blood. These tests screen for indicators that may demonstrate the presence of cancer, such as:
- Anaemia (too few red blood cells; caused by internal bleeding or a lack of enough production of red blood cells, a common cancer symptom)
- Polycythaemia (too many red blood cells; sometimes caused by cancerous tumours in the kidney that trigger the release of EPO, a hormone that increases red blood cell production in bone marrow)
- Hypercalcaemia (high blood calcium levels) and elevated liver enzymes (conditions characteristic of RCC)
Treatments for Kidney Cancer
There are a number of treatment options for kidney cancer; the ideal treatment depends on a number of factors, including the extent of the tumour and the current health of the patient.
Treatment options vary and these should be discussed with Dr Kim to identify which is the best course of treatment for each individual patient.
They include active surveillance, surgery, focal ablative therapy, systemic or immunotherapy and radiation therapy.
Radical Nephrectomy
The most common form of surgery for renal cell carcinoma (RCC), radical nephrectomy involves removal of the entire kidney, sometimes along with the attached adrenal gland, surrounding fatty tissues and nearby lymph nodes (regional lymphadenectomy), depending upon how far the cancer has spread.
Partial Nephrectomy
It may be possible to remove only the cancerous tissue and part of the kidney if the tumour is relatively small and is deemed to be technically safe and feasible.
A partial nephrectomy is the procedure of choice for patients with RCC in both kidneys and for those who have only one functioning kidney. Partial nephrectomy is associated with better preservation of long term renal function compared to removing the entire kidney. This is certainly the case if a patient has other diseases that can affect kidney function in the future (such as high blood pressure, diabetes), or if the opposite kidney is not working properly, has never formed or has already been removed.
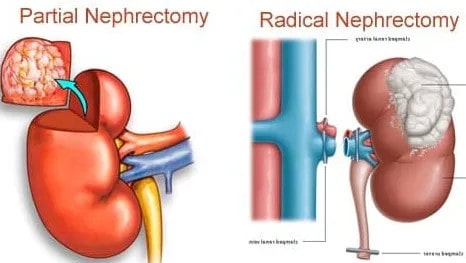
Partial Nephrectomy vs Radical Nephrectomy
Robotic and Laparoscopic Radical Nephrectomy and Partial Nephrectomy
Robotic and laparoscopic techniques allow the kidney to be removed using key-hole incisions in the abdomen. Conversion to the standard open operation can be safely accomplished, should technical difficulty be encountered.
Laparoscopic surgery uses hand-held key-hole instruments while the robotic surgery provides a 3-D magnified view with wristed instruments that are easier to manipulate with more precision than standard hand-held key-hole instruments.
A standard laparoscopic approach using the hand held keyhole instruments is often sufficient for a radical nephrectomy. In comparison, a partial nephrectomy is more complex and so using the robot can arguably help make the operation easier to perform.
Radiotherapy
Radiation in the form of X-rays or other high-energy rays is used to shrink and kill cancer cells in some kidney cancer patients. The radiation is delivered as a focused beam (external beam radiotherapy) that is projected into the body through a linear accelerator.
Radiation therapy can be used as palliative therapy to lessen pain or bleeding in patients with inoperable or widespread metastatic RCC.
Follow-up Care and Recurrent Kidney Cancer
Some patients who undergo surgery to remove a cancerous kidney or kidney tumours experience a recurrence of the disease. For this reason, patients usually undergo a regimen of follow-up examinations after surgery.
These include:
- Complete physical examination,
- Complete blood tests (including kidney function)
- Scans (ie. chest X-ray, ultrasounds, CT, MRI, or PET)
If the disease recurs but remains confined to a few small areas, additional surgery may be recommended.
Other non-surgical treatments include:
- Radiation,
- Targeted systemic therapy or immunotherapy also may be tried as an adjuvant or palliative (for symptom relief) treatment. (Chemotherapy would not work for kidney cancer.)
What are the Consequences if Kidney Cancer is Untreated?
Kidney Cancer is a serious condition and if left untreated, kidney cancer can potentially progress and spread to other areas of the body, such as the bones, lungs or even brain.
Therefore, as with other types of cancer, early detection is important for improving the likelihood that treatment will be effective. Untreated Kidney Cancer can result in significant negative impact on quality of life and even death.